

With pressures only intensifying on clinical trials, there are major concerns that current models are inefficient and unsustainable.
Insight from recent GlobalData reports and industry analyses expose a system under immense strain. More trials are open than ever before, but there are fewer people and resources available to conduct them. Costs are increasing, timelines are stretching, and the patients these trials are meant to help are left waiting for treatments that may never arrive.

Without urgent reform, the clinical trial enterprise as we know it cannot continue.
The rising volume of clinical trials increases demand and competition for patients
The number of oncology assets in the clinical development pipeline has increased by 13% annually over five years (2018-2022)1. On paper, this sounds like a positive time for medical innovation. However, growth at this rate will more than triple the demand for patients to enroll in clinical trials by year 20322. The present clinical trial ecosystem is not equipped nor projected to have the capacity to satisfy this demand, and as a result the ecosystem is facing a potential slowdown in drug development.
More study sites are needed to run trials, more trials will need to be run at each site, and each study site will need to achieve greater enrollment productivity to mitigate a looming global slowdown in drug development.
A dwindling clinical trial workforce that is overworked and burning out
Over 80% of research sites in the United States have faced staffing shortages in oncology clinical research, largely attributed to unsustainable job expectations, lack of adequate compensation, and limited career growth potential.3
GlobalData’s analysis shows that the number of clinical trial investigators globally fell from approximately 128,303 in 2017-18 to 116,948 in 2023-24 – a decline of almost 10%. The ranks of trial site coordinators dropped even more steeply in these periods, dropping from approximately 56,036 to 40,472.
Many research and healthcare workers left the field after COVID-19, explains Kent Thoelke, CEO of Paradigm Health. “There was an exodus post-COVID,” he says. This means that startup times for new clinical studies are lengthening as sponsors search for investigators with capacity at a time when that very capacity is falling. Unless actions are taken to reduce the burden and inefficiencies impacting this workforce, this trend will continue to worsen.
Alongside this falling workforce are struggles with participant recruitment for clinical trials. The leading cause of trial termination remains inadequate patient levels, with more trials being abandoned due to lack of enrollment than for any reasons e.g., safety or efficacy. Industry data indicates that roughly 60%-70% of trial sites failed to enroll their initial targeted patient numbers. Furthermore, the costs to initiate and manage those non-enrolling sites – such as contracting, training, and overhead – are wasted.
Academic medical centers continue to conduct the bulk of trials, especially in the US, while community hospitals and clinics often lack the resources to participate in trials at scale. This is despite the majority of patients being treated at community hospitals and clinics.
According to Thoelke, only approximately 5%-8% of potentially eligible patients ever take part in a clinical trial, a figure that has remained stagnant for years. With such low participation rates, there is no viable path to fulfill the growing demand for patients to enroll in trials.
Areas underserved by clinical trials
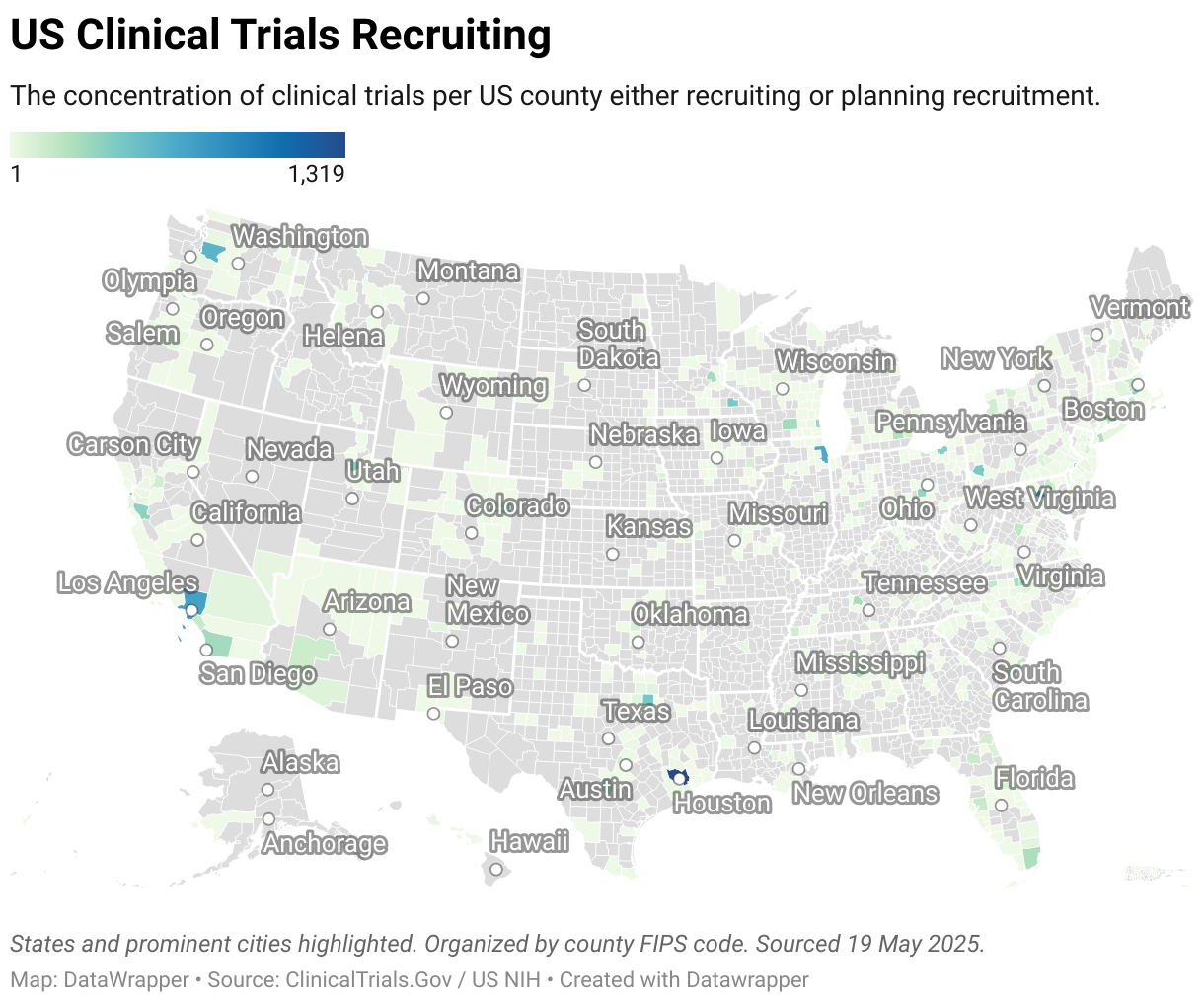
According to the ClinicalTrials.gov, almost 26,000 clinical trials were recorded to be seeking participants across all 50 states in the US in May 2025. Some states were far busier than others. Unsurprisingly, the coastal states with large urban centers were recruiting the highest number of participants.
A map of trial recruitment activity across US counties paints a stark picture, with large stretches of the country not recruiting for clinical trials at all.
All of this means that patients living in more rural communities are effectively shut out of the majority of clinical trials. Whether clinical trials that are recruiting will reach enrolment targets remains to be seen, given the long-term issues with recruitment.
Research by the Milken Institute estimates that people living in agricultural counties are likely to travel more than 60 miles to participate in a clinical trial than people who live in an urban environment or affluent suburbs.4
States with smaller patient pools risk oversaturation or exhaustion, but there is a real risk of total exclusion from clinical trials for rural communities. Thoelke explains that as treatments become more personalized to specific genetic markers or subpopulations, the patient pool shrinks.
“Research staff can spend a significant amount of time sifting through medical records to find the patients under care that fit incredibly specific trial criteria,” he says.
In prevalent cancers – such as lung and breast – there are numerous competing trials vying for the same pool of eligible patients. The result is that each trial enrolls an inadequate number of participants, prolonging recruitment for each trial or leaving one or more trials completely unable to meet enrollment targets.
Oncology may be at the forefront of this issue, but other therapeutic areas are also feeling the strain. Trials in chronic conditions such as Alzheimer’s disease and other CNS disorders face notorious recruitment challenges, often because patients are treated in rural community settings that are not equipped to run clinical trials.
Rare disease trials, by definition, struggle with small patient pools scattered across the globe. Yet even in these areas, the volume of trials is increasing as scientific advances open new possibilities without a corresponding progress in how patients are found and enrolled. Relying on a on academic medical centers and expecting rural patients to travel or disrupt their lives to join a trial is leading to diminishing returns.
Trials intended for FDA submission must include patients representative of the US population
While clinical trials can be conducted in multiple regions throughout the world in order to increase the pool of eligible patients, the proportion of US patients in applications submitted to the US FDA has been declining. While FDA may accept clinical data from ex-US sites, the enrolled population has to be applicable to the US population and medical practice.
A recent oncology drug advisory committee voted against approval of one drug based on concerns that the ex-US data was not applicable to the US population.5 Thus, in addition to an increase in demand from the developmental pipeline, there is a renewed focus on increasing the component of US participation in registrational trials.
For all these reasons, increasing access and reducing burden to trial participation at US sites is critical to bringing novel treatments to patients.
The rising cost of clinical trials
Clinical trials have always been expensive, but costs are reaching new heights. According to a November 2024 GlobalData report, per-trial costs have risen steadily since 2014, with single country trials increasing by 2.9% per year and multinational studies rising by 4.9% per year over this decade.
Oncology trials are particularly expensive, averaging ~$30m per Phase 1 trial and nearly $60m for a Phase 3 trial6, with the largest trials exceeding $100m in direct costs.
High and rising direct trial costs are the result of increased complexity of clinical trials (more complex treatment regimens, more adaptive trial designs, more expansive data collection, and more protocol amendments) combined with declining productivity per trial and per site (fewer enrolled patients per site per month, leading to extended recruitment durations.7
For sponsors, longer trial timelines mean higher direct trial costs. Every month that a trial remains open without results, sponsors must pay for additional site maintenance, monitoring, and administration, amounting to $40,000 additional cost per day.8
To make matters worse, longer trial timelines delay the launch of new therapies, imposing substantial additional costs on sponsors. For each day of delayed drug launch, sponsors forego an average of $500,000 in lost drug revenue8, a figure that can exceed $3m per day for a blockbuster drug with >$1bn annual sales.
This lost revenue is all the more painful to sponsors in an era of shortening periods of market exclusivity, particularly for small molecule drugs in the US due to changes enacted in the 2022 Inflation Reduction Act.9
Rising direct trial costs and lost revenue due to delayed approval are key factors driving the total cost of bringing a new drug to market to a staggering $2.3bn.10
“That is simply unsustainable,” Kent Thoelke argues, especially as drug pricing pressures mount in major markets. If trials continue to be conducted in the same costly way, fewer drugs will be economically viable to develop. The return on investment is shrinking, and some sponsors may be forced to abandon promising therapies because the development costs are simply too high.
The cost of single-Country vs. multinational trials in the US

Source: Globaldata.
Why a different model is required for clinical trials
The unsustainability of the current system and outdated patient enrollment methods are fueling a search for transformative models. Thoelke and others believe the answer lies in re-engineering the clinical research model. The pandemic provided a glimpse of this future. When COVID-19 struck, many rigid trial protocols were relaxed out of necessity. Patients could give consent electronically, provide samples at local labs, or participate from home via telemedicine.
What industry had resisted for years, a global crisis achieved in months: a shift toward expanding patient access to clinical trials.
“This allowed us to continue participation in clinical trials for patients that were on lifesaving therapies during the pandemic,” Thoelke explains. “But most of those systems rolled back, we’ve gone back to the status quo.”
Addressing inefficiencies in clinical trials
Paradigm Health’s AI-driven platform addresses longstanding inefficiencies in identifying and recruiting eligible patients, as well as reduces the data collection burden that is especially taxing on the research staff in community care settings.
“The process for running clinical trials has not dramatically improved in three decades,” Thoelke explains. “We need to reengineer the research model with new technology and infrastructure that equips community and rural healthcare systems to participate in clinical trials at greater scale.”
“Our AI platform interprets the entirety of [the patient’s] chart, matches the patient to trials, and collects the data for a trial with far less manual burden on the research staff. We can quickly read massive volumes of records with high levels of precision.”
This is not just about technology, it’s also about accessibility and equity.
The consequence is that many patients, especially outside major cities, cannot access cutting-edge trials, even if it’s their best care option. Paradigm Health has shown that community healthcare providers can run complex oncology trials with the right support, giving rural patients the same opportunity as those at academic medical centers concentrated in large cities.
To serve both science and patients, the industry must embrace transformation before inefficiency puts progress out of reach.
To learn more about the solutions provided by Paradigm Health, download the document below.
References:
1. Li B. Bloomberg New Economy International Cancer Coalition, McKinsey Cancer Center, Cure4Cancer; Advancing Global Health Equity in Oncology Clinical Trial Access. Cancer Discov 1 December 2024; 14 (12):2317–2323. https://doi.org/10.1158/2159-8290.CD-24-1288
2. GlobalData analysis based on active interventional Ph1-3 oncology trials and average patient enrollments by phase. (2025)
3. Sun G, et al. Crisis of the Clinical Trials Staff Attrition After the COVID-19 Pandemic. JCO Oncology Practice, Volume 19, Number 8, June 2023, https://ascopubs.org/doi/10.1200/OP.23.00152
4. Friedson A, et al. Distance as an Obstacle to Clinical Trial Access: Who Is Affected and Why It Matters. Milken Institute. Research and Data Tools. June 2024. https://milkeninstitute.org/contenthub/research-and-reports/research-and-data-tools/distance-obstacle-clinical-trial-access-whoaffected-and-why-it-matters
5. James D. FDA Panel Votes Against Columvi-GemOx sBLA for R/R DLBCL Over Regional Data Concerns from STARGLO Trial. Applied Clinical Trials. May 2025. https://www.appliedclinicaltrialsonline.com/view/fda-panel-columvi-dlbcl-starglo-trial
6. Sertkaya A, Beleche T, Jessup A, Sommers BD. Costs of Drug Development and Research and Development Intensity in the US, 2000-2018. JAMA Netw Open. 2024;7(6):e2415445. doi:10.1001/jamanetworkopen.2024.15445
7. Agrawal G, et al. Accelerating Clinical Trials to Improve Biopharma R&D Productivity. McKinsey & Company. Views from McKinsey’s Life Sciences Practice. January 2024. https://www.mckinsey.com/industries/life-sciences/our-insights/accelerating-clinical-trials-toimprove-biopharma-r-and-d-productivity
8. Smith ZP, DiMasi JA, Getz KA. New Estimates on the Cost of a Delay Day in Drug Development. Therapeutic Innovation & Regulatory Science. 2024 Sep;58(5):855-862. doi: 10.1007/s43441-024-00667-w. Epub 2024 May 21. PMID: 38773058. https://link.springer.com/article/10.1007/s43441-024-00667-w
9. Cubanski J, et al. Explaining the Prescription Drug Provisions in the Inflation Reduction Act. KFF. January 2023. https://www.kff.org/medicare/issue-brief/explaining-the-prescription-drug-provisionsin-the-inflation-reduction-act/
10. Philippidis A. The Unbearable Cost of Drug Development: Deloitte Report Shows 15% Jump in R&D to $2.3 Billion. GeneEdge News. February 2023. https://www.genengnews.com/gen-edge/the-unbearable-costof-drug-development-deloitte-report-shows-15-jump-in-rd-to-2-3-billion/
